






Unsheltered individuals manage profound health challenges that broadly define them as a social group. This is the basic conclusion of a recent California Policy Lab (CPL) brief—Health Conditions Among Unsheltered Adults in the U.S.
In the lead up to the publication, unsheltered homelessness was on the rise. It increased by 12 percent between 2015 and 2018—even as overall homelessness was on the decline. Experts, wanting to understand the reasons for this trend, began asking questions that included: How are unsheltered individuals different from sheltered ones? CPL examined responses from the Vulnerability Index—Service Prioritization Decision Assistance Prescreen Tool (VI-SPDAT), a survey given to people experiencing homelessness, in search of answers.
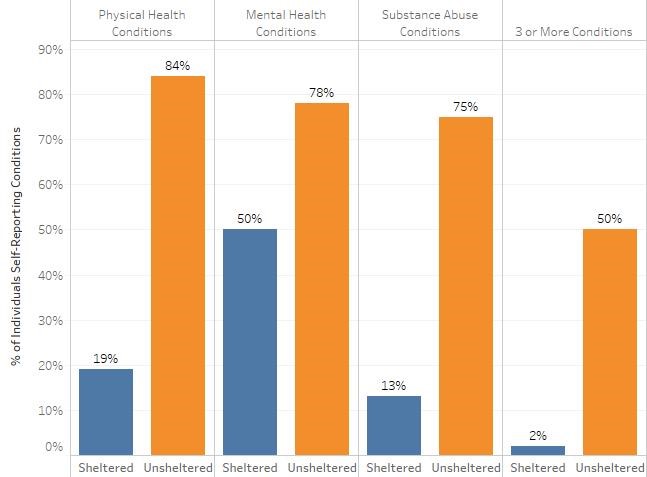
According to CPL’s findings, unsheltered individuals have more significant health challenges than their sheltered counterparts. For example, 84 percent of unsheltered individuals report physical health conditions compared to just 19 percent of sheltered individuals. Significant gaps between the two groups also exist in the areas of mental health and substance abuse.
These unsheltered adults were much more likely to say that their health conditions contributed to their loss of housing.
Most homeless individuals are men. However, this research raises significant red flags related to Domestic Violence Awareness month. Not only did women report greater health challenges, but eighty percent of unsheltered women said abuse and/or trauma contributed to their homelessness. This is far higher than the numbers of unsheltered men (38 percent) or even sheltered women (34 percent) who said the same.
Current Responses
How are communities responding to this health crisis?
Clearly, shelters and housing programs are not adequately reaching unsheltered people. Unsheltered people go longer periods of time without stable housing than sheltered people do—an average of 2,632 days, compared to 410 days for sheltered individuals. And they don’t spend many nights of the year in shelter—this is especially true for women.
Law enforcement is reaching this group, however. Unsheltered individuals report ten times as much police contact in the previous six months when compared to sheltered individuals. And they are more likely to spend nights in jail.
These are not ideal solutions to a health crisis.
Next Steps in Solving a Crisis?
Solving a health crisis requires the leadership of healthcare systems, providers, and researchers. Three next steps include:
Improving outreach: Doctors and other health professionals must improve their outreach to people experiencing unsheltered homelessness to fully address their needs. This would promote well-being while helping to confront the causes of homelessness. Similarly, healthcare professionals must play a more significant role in homelessness prevention, which should include anticipating and treating health needs before they lead to a loss of housing.
Reducing barriers to shelter and housing. Access to shelter and housing will save lives. In the short term, shelter minimizes exposure to the elements. Over the long term, permanent housing stabilizes people and allows them to consistently participate in medical treatment. Homeless and housing providers must examine why unsheltered homeless individuals are not accessing temporary and permanent housing services. The Alliance regularly offers materials that help providers 1) reexamine shelter rules that create barriers to access and 2) focus more attention on permanent housing outcomes.
Continue the discussion. Finally, researchers should consider next step research questions. For example, recent data warrants a closer look at unsheltered women. What more can be learned about the status of their health? And why aren’t survivors of abuse and trauma accessing shelter and other housing assistance? More detailed examinations into subsets of the unsheltered population can lead to solutions in addressing this health crisis.
You might also be interested in






Stay Updated: Solutions, Stories, and Ways to Make an Impact
Sign up to receive updates on the Alliance’s work, including the latest research, advocacy efforts, and real stories of progress — plus ways you can help drive lasting change.